Thursday
Dec292011
Speculative Environments: Spaces of Disease Surveillance
By Lindsay Thomas
[ PDF version ]
The global surveillance of infectious disease is fundamentally connected to problems of scale: how to track the movement of contagions through different populations and across regional and national boundaries requires the negotiation of scales ranging from the molecular to the global. Often such negotiation is most successfully carried out through the use of geographic information systems (GIS), information systems that are a combination of digital cartography, database management, and spatial analytical tools. This essay concerns two GIS used for disease surveillance: the World Health Organization’s (WHO) FluNet, part of its Global Influenza Surveillance and Response System (GISRS), and the National Infrastructure Simulation and Analysis Center’s (NISAC) Epidemic Simulation System (EpiSimS), an agent-based simulation engine for modeling the spread of infectious diseases through different regions of the United States. Through their negotiation of a wide range of scales, these systems construct spaces of disease surveillance—environments governed less through empirical modes than through speculative modes. Disease surveillance using GIS, then, points to a greater shift in how governments, particularly the government of the United States, enact security.
One method of disease surveillance is performed through institutional infrastructures constituted by interconnected biotechnological networks dedicated to disease surveillance. One such network is the GISRS, the WHO’s oldest and most extensive global disease surveillance network. Operational since 1947, the GISRS today is composed of 135 National Influenza Centers (NIC) in 105 different countries that annually collect more than 175,000 patient samples containing over 2,000 discrete strains of influenza. The NICs send these samples to one of six WHO Collaborating Centers (CC) — located in Australia, China, Japan, the United Kingdom, and the United States — and these centers analyze the virus samples to determine whether influenza viruses currently in circulation differ significantly from viruses for which a vaccine already exists. Using this data, the WHO CCs are able to make biannual recommendations for influenza vaccine formulations. In this way, the institutional network of the GISRS monitors the evolution of existing influenza viruses and tries to detect the emergence of new strains, serving “as a global alert mechanism for the emergence of influenza viruses with pandemic potential.”[1]
Serving “as a global alert mechanism” for influenza pandemics requires the systematic communication of information about the spread of the virus as well as the number and type of virus samples gathered and vaccines created. To this end, the NICs and CCs make the information they gather and collate available to public health officials and other interested parties using the GISRS’s main tool for information sharing: a web-based tool called FluNet that captures, stores, analyzes, manages, and presents geographic, epidemiological, and virological information on influenza. FluNet brings together data on the influenza virus, its movement through particular populations, and the kinds of resources — including health care facilities and transportation and information-infrastructures — available to these populations. Data entry is restricted to officials associated with certain NICs and WHO CCs but certain data is available to all public users in the form of charts, graphs, and maps. Although data updates are only required once weekly, FluNet allows public health officials access to recent data on the status of the influenza virus, data that is potentially useful when trying to monitor or prevent the spread of influenza.
Another form of disease surveillance is carried out by NISAC, a division of the Department of Homeland Security composed of personnel located in Washington, D.C. at the Sandia National Laboratories and at the Los Alamos National Laboratory in New Mexico. One of the many simulation tools utilized by NISAC is EpiSimS, a C++ application that models the daily movements and interactions of synthetic individuals within a city or region and creates social networks representing these interactions. It then combines these social networks with models of the geographic spread of disease in order to deliver models of the demographic and geographic distributions of a particular disease; in other words, this application offers an agent-based model within a targeted geographic information system environment. Like FluNet, it maps the spread of disease over geopolitical, topographical, and transportation system maps. What’s more, due to its high level of granularity, EpiSimS, unlike FluNet, is able to provide data on relatively small geographic regions like counties and cities. This “provides decision makers with information about (1) the consequences of a biological attack, (2) the resulting demand for health services, and (3) the feasibility and effectiveness of response options.”[2] Much like FluNet, EpiSimS’s output is in the form of charts, tables, and scalable maps. Unlike FluNet, however, data input and output is restricted to experts and public health officials; most of the simulation models and information produced using EpiSimS are not publicly available. One of the many ways in which officials at NISAC have used EpiSimS is through the modeling of the spread of pandemic influenza in several counties in southern California. Performed in 2007, this model provided information on how best to control the spread of pandemic influenza using a multi-component strategy involving both pharmaceutical — the distribution of stockpiled vaccines — and non-pharmaceutical — school closures and work absenteeism — intervention strategies.[3] Some of these strategies were then utilized during the 2009 H1N1 pandemic.[4]
As surveillance systems, FluNet and EpiSimS are evidence of the militarization of public health. They aspire to a totalizing vision that maps the micro-scale of viral infection onto the macro-scale of geopolitics. Ideally, this kind of scalar negotiation allows officials to prepare for the emergence of infectious disease, detect this emergence when it occurs, and direct resources toward containing the spread of such diseases. In other words, these systems attempt to articulate control within the emergence of unpredictable networks of infection.[5] This essay is an exploration of this articulation; attention to the history and mechanics of the hybrid spaces created by geographic information systems like FluNet and EpiSims provides both an investigation of the knowledge produced by these systems and a case study of the ways in which media negotiate complex problems of scale. Such negotiation, as we will see, is crucial to how these systems build, naturalize, and govern fundamentally speculative environments.
Scale and Security
The totalizing vision of geographical information systems is made possible by the density of their perceptual fields. Concerned with tracking and visualizing epidemiological and virological data as well as infrastructural and geological topologies, FluNet and EpiSimS allows users (public or private) to create maps that layer the networks of bodies, institutions, and transportation and communication technologies through which viruses and information about viruses travel.[6] In FluNet, for example, users can add a wide variety of layers to geopolitical base maps. They can select “Indicators” to be displayed, which include the distribution of certain communicable and noncommunicable diseases, the distribution of human resources for health like community and traditional health workers and nursing personnel, and world health statistics on risk factors and basic demographic information. Users can also select which “Core Layers” they would like to display; these include information about infrastructures like roads, ports, and health and education services and information on the location of natural features and water services. Similarly, EpiSimS creates regional maps that include geopolitical features like county and city borders and highway systems, and epidemiological information like the spread of disease or rate of infection. In this way, FluNet and EpiSimS map the molecular level of viral infection onto densely layered regional, national, and global scales. The base unit of measurement in these maps is that of population distributed across a regional or national space, and, importantly, across a certain amount of time; relations of contagion and transmission — incidences of infection, for example — are mapped at the level of the population contained within geopolitical boundaries and the standardized space and time of the coordinate grid. These maps, then, create hybrid spaces composed of aggregate human-nonhuman interactions and scales organized around a densely layered and totalizing perceptual field.
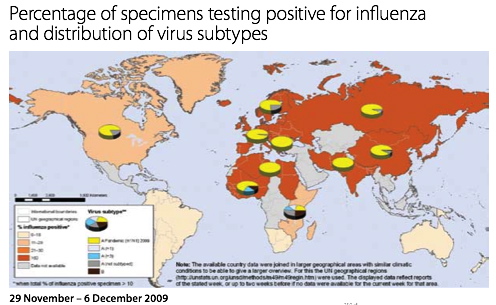
Figure 1. FluNet influenza map. Source: “Evolution of a Pandemic”[7]

Figure 2. EpiSimS influenza map. Source: “NISAC Tools: EpiSimS”[8]
In this way, geographic information systems are certainly technologies of what Foucault calls governmentality, or “governmental management, which has population as its main target and apparatuses of security as its essential mechanism.”[9] Apparatuses of security rely not on the prohibition of events but rather on the calculation of their probability and the regulation of their occurrence, the two main functions of both FluNet and EpiSimS. Dealing with what is given or factual, such apparatuses “work within reality, by getting the components of reality to work in relation to each other, thanks to and through a series of analyses and specific arrangements.”[10] This involves equating the molecular scale of viral infection to regional, national, or global scales, or mapping them both within the same standardized space and time through statistical analyses. These GIS are apparatuses of security that manipulate a vast range of scales so that they occur on the same plane; the densely-layered fields of vision that comprise these spaces are made to appear flattened and total. Due to the relatively long amount of time they represent — a day, week, month, year — the maps simultaneously position past duration as instantaneous and future time as probabilistic. Security, then, is fundamentally related to the manipulation of many different spatial and temporal scales so they can appear within the same environment.
Constructing Disease Environments
This kind of manipulation has, historically, been the combined project of medical geography and, later, epidemiology. The emergence of the field of medical geography, most often associated with the publication in 1792 of two volumes of German physician Leonhard Ludwig Finke’s three-volume Versuch einer allgemeinen medicinisch-praktischen Geographie (An Attempt at a General Medical-Practical Geography), largely regarded as the first major medical geography text, was in part made possible by a miasmatic theory of disease (from miasma, Greek for “contamination”). A precursor to the germ theory of disease, this theory understood disease to be caused by the noxious air of particular places. It can be traced as far back as Hippocrates in Western medicine, and it prevailed as the dominant understanding in the West of how disease was caused and transmitted until the end of the nineteenth century. In miasmatic theory, contamination rather than contagion was the dominant model of disease transmission: it was not people but rather places that were sick and that could transmit disease. As a result, “the focus of medical attention consequently shifted away from anatomy to ecology, from the study of the body as the locus of disease to the analysis of the disease-bearing aspects of physical environments.”[11] Medical geography made possible, then, “a radical medicalization of global space: the mapping of the entire world in terms of disease.”[12] This project was important, among other things, to the British colonial project and the legacy of public health practices the British left behind in their former colonies.[13]
What we see in the history of medical geography, unsurprisingly, is an emphasis on the spatial environments in which diseases occur and through which they spread. Even from the mid- to late-nineteenth century, after the germ theory of disease was largely accepted, the relationship of disease to place remained paramount in the new discipline of epidemiology. London physician John Snow’s well-known maps of the 1852 cholera outbreak are, in this way, a kind of turning point. Published in 1854 and 1855, these extraordinarily rigorous distribution maps, dependent on the increasingly common use of statistics in epidemiology, demonstrate the incidence of cholera infection occurring in London’s Broad Street neighborhood. Using these maps, Snow pointed to the cause of the cholera outbreak: a pump used by many Broad Street residents was infected with cholera by a sewage pipe discharging its contents next to the pump well. This insight “served to critique, at least implicitly, the miasmatic theory of airborne disease, which, if correct, [Snow] noted, would result in a uniform pattern of incidence rather than the intense variations he had observed street by street and house by house.”[14] These intense variations were due to the differences in the places where residents and businesses obtained their water; Snow’s maps thus pointed to the idea that cholera was a waterborne, not an airborne or place-specific disease. No longer associated with depicting specific places as the determinant cause of disease, as miasmatic theories of disease would have it, Snow’s maps pointed instead to the statistical correlations between diseases and places. Such probabilistic calculations, again, highlight the spatial distribution of diseases throughout a particular time or times, or the patterns in which diseases spread or diffuse through the environment.
This shift evidences a different understanding of what constitutes an “environment.” Like Snow’s maps, FluNet’s maps relate the health of particular populations to the spaces they inhabit. In other words, through this negotiation of a vast range of scales, they create hybrid human-nonhuman spaces that enfold individuals and population, population and place. To use Nigel Thrift’s terminology, their “content is the bending of bodies-with-environments”;[15] they blur distinctions between bodies and their environments, creating new techno-biopolitical spaces of viral infection, information and transportation networks, and geopolitical boundaries. Composed of data that is both individual and aggregate, both mobile and singularly locatable within a standardized coordinate grid, these paradoxical maps are of course highly artificial and unnatural representations. They are maps of mathematical models concerning actual disease distribution and spread over a certain amount of actual time; in other words, they attempt to project the real-time transformation of data within the space of a static representation.
Yet these maps also evidence a kind of “re-naturalization” of constructed spaces. As Thrift writes, “increasingly, the ‘artificial’ environment is sentient and has the feel of a set of ‘natural’ forces blowing this way and that.”[16] Nowhere is this more evident than in the environments created by FluNet. As we see in Fig. 1, certain places are “sicker” than others; there are no distinctions made between the sick population of a particular country — measured using the number and type of influenza virus subtypes occurring in a particular country — and its geopolitical characteristics. Bodies are enfolded, automatically and according to the parameters of the system, into the country in which they reside; the rate and spread of infection is represented according to paradoxically “natural” — because they are representative of reality and because they occur automatically, according to the parameters of the system — calculations. Such an understanding of environment emphasizes spaces of interaction, spaces where time continually unfolds, over totalizing vision. While FluNet is a primary tool of disease surveillance, the spaces it creates can also be seen as stages on which new and unanticipated interactions may take place. By emphasizing what such maps perform — the spatial formations and enfoldings they enact and anticipate — rather than what they represent, we are perhaps confronted with a different mode of governance, a mode more speculative than representational.
Performing the Unknown
The models created using EpiSimS are evidence of this mode. These maps are performances, created according to the rules of the simulation. The maps of the spread of pandemic influenza in southern California, for example, were created using population data from the 2000 census. The population modeled consisted of 18.8 million individuals living in 6.3 million households, with an additional 938,000 locations representing actual schools, businesses, shops, or restaurant addresses.[17] Each person or agent in the simulation was given a schedule of activities to do during the day, comprised of nine possible activities: home, work, shopping, visiting, social recreation, passenger server, school, college, and other. As the agents went about their days, they encountered one another at various locations, which were further divided into rooms or mixing groups; disease transmission could only occur between agents who occupied the same room of a location at the same time, but not all agents who happened to be at the same location at the same time were close enough to transmit disease. Infected agents could pass through fourteen possible disease states, and because “the epidemiology of the future influenza virus [was] not known” and would “not be known until it emerge[d],” the “influenza disease model [was] based on historical data and previous epidemic models.”[18] In other words, the types of disease states through which agents passed — non-infectious incubation, pre-symptomatic infectious, symptomatic-infectious, asymptomatic-infectious, etc. — and how long they remained in these states was calculated using historical data on pandemic influenza. These maps, then, evidence not only the bending of bodies-with-environments and the re-naturalization of these environments, but also a mode of knowledge built on speculation, on the extrapolation of known events and data from the past or present into the future.
Such practices are part of a larger historical shift in how the U.S. government practices security, precipitating an emphasis on preparedness and resilience by emphasizing how to prepare for and respond to the catastrophic. Andrew Lakoff is paradigmatic of those scholars who have investigated this shift, emphasizing what he terms vital systems security. This form of security, which he traces back to the United States government’s practice of civil defense in the mid-twentieth century at the beginning of the Cold War, is concerned with a particular kind of threat, a threat that is potentially catastrophic yet fundamentally unknowable because its probability and form cannot be calculated. This kind of security focuses not on “the national territory or the population but rather the critical systems that underpin social and economic life.”[19] Vital systems security does not develop knowledge about a foreign enemy or about regularly occurring events; rather, it “uses techniques of imaginative enactment to generate knowledge about system vulnerabilities.”[20] Speculation, then, is its mode of knowing. Vital systems security stresses a rationality of preparedness in which catastrophic scenarios are imagined and enacted in order to seek out weaknesses in certain critical systems infrastructures. Because this rationality of preparedness does not deal with the calculation of future probable events but rather with events that are incalculable and as likely to happen at one time as they are at another, like pandemic influenza, “preparedness does not prescribe avoidance…. [it] does not seek to prevent the occurrence of a disastrous event but rather assumes that the event will happen.”[21] A rationality of preparedness “enacts a vision of the dystopian future” in order to expose system vulnerabilities and attempt to mitigate them in preparation for the occurrence of the very dystopian future it simulates.[22] The rationality of preparedness that is taken up in vital systems security is concerned with the simulation of future catastrophic events, events it sees not merely as probable but instead as certain.
EpiSimS is a simulation engine created exactly for this purpose; built and operated by trained officials at NISAC, it produces expert knowledge about how public health officials can prepare themselves, their staff, and the infrastructures and information networks of which they are a part for pandemic influenza. Using historical data, it simulates infectious disease pandemics not in order to prevent them from emerging but rather in order to prepare for their occurrence. The calculations it performs shift past probabilistic data on rates of infection and disease distribution into a simulated future that is also of course unfolding in the present. In this way, although they are based on the probability that future epidemics will behave like those in the past, EpiSimS nevertheless operates outside the realm of probability. Its form of knowledge production is speculative, a type of partial knowledge that, in its managerial forms, obscures its own conjectural modes. It maps the future as a series of unknowns naturalized as probabilities, it predicts always-coming possible harm, and it enacts worst-case scenarios to try to bring what are fundamentally spectacular projections under the rubric of the known. EpiSimS, then, points not to surveillance as a mode of governance but rather to speculation. The future, so it can be known, is mapped according to data from the past, and the present time of the simulation is projected at once backward to the past and forward to the future. Time is not frozen in a static representation but rather extrapolated backwards and forwards. Maps built with EpiSimS are not so much representations of reality as they are performances of possible future realities based on the past; they are constructed environments literally built on interaction that feel, once they are enacted, all too familiar, natural and inevitable — as if they had happened before.
FluNet and EpiSimS, as two modes of disease surveillance, point to the complicated ways in which media like GIS engage with issues of spatial and temporal scales. This engagement is important not only to a consideration of the kinds of environments these media construct, but also to a consideration of the modes of governance they produce and within which they operate. While much work on GIS and disease surveillance has focused on the representational strategies of these systems — the ways in which they represent the world in order to survey it — this essay has, in part, been a speculation on their performative nature. Concerned with the enactment of the unknown, these geographical information systems emphasize changing conceptions of what it means to interact with one’s environment, and at what scale. For the institutions discussed here such interaction is increasingly speculative. Borrowing from the realm of fiction, such concrete imaginings of the future play out daily in the hybrid environments built by these geographic information systems.
Notes
[1] “WHO Global Influenza Surveillance and Response System,” World Health Organization Global Alert and Response, accessed 9 Dec 2011, http://www.who.int/influenza/gisrs_laboratory/en/.
[2] “Epidemiological Simulation Systems (EpiSims),” National Infrastructure Simulation and Analysis Center, accessed 17 July 2011, http://www.sandia.gov/nisac/episims.html.
[3] See, for example, Susan M. Mniszewski, Sara Y. Del Valle, Phillip D. Stroud, Jane M. Riese, Stephen J. Sydoriak, “EpiSimS Simulation of a Multi-Component Strategy for Pandemic Influenza,” SpringSim ’08: Proceedings of the 2008 Spring simulation multiconference (2008): 556-563, accessed 17 July 2011, http://public.lanl.gov/sdelvall/p556-mniszewski.pdf.
[4] “In late April 2009, the U.S. Government declared a public health emergency due to an outbreak of novel influenza A (H1N1). NISAC…provided analysis support to decision makers by responding to immediate requests for information on diverse issues such as border closure impacts, economic impacts of travel restrictions, and potential overloads to the nation's healthcare system. NISAC generated new analysis results within a timeframe of days, drawing on relevant information from its more extensive 2007 H5N1 pandemic influenza study and fast-response analysis. NISAC's results were used to inform DHS senior leadership.” “Pandemic Influenza Modeling,” Los Alamos National Laboratory, accessed 20 July 2011, http://www.lanl.gov/programs/nisac/products/pandemic.shtml.
[5] Eugene Thacker writes, “The challenges put forth in this tension between ‘control’ and ‘emergence’ are not just technical problems, but are challenges that raise ontological as well as political questions. From the network perspective, case studies like the 2003 SARS epidemic look very much like a centralized information network counter-acting a decentralized biological network. The WHO’s outbreak response network coordinated the exchange of data through network servers and conference calls, and health advisories could then radiate from this central node. By contrast, SARS infection was maximized by moving through the highly-connected nodes of airports and hotels. The strategy of DSNs, then, is to canalize transmission in order to fight the decentralization of contagion. If an epidemic is ‘successful’ at its goals of replication and spread, then it gradually becomes a distributed network, in which any node of the network may infect any other node.” See Thacker, “Living Dead Networks,” Fibreculture 4 (2005), accessed 20 July 2011, http://four.fibreculturejournal.org/fcj-018-living-dead-networks/.
[6] As many have noted, a virus and information about a virus are, effectively, the same thing. See Alexander R. Galloway and Eugene Thacker, The Exploit: A Theory of Networks (Minneapolis: University of Minnesota Press, 2007), 87, 88.
[7] World Health Organization, Evolution of a Pandemic: A(H1N1) 2009 (Geneva: WHO, 2010), http://whqlibdoc.who.int/publications/2010/9789241599924_eng.pdf.
[8] “NISAC Tools: EpiSimS,” Los Alamos National Laboratory, accessed 17 July 2011, http://www.lanl.gov/programs/nisac/episims.shtml.
[9] Michel Foucault, Security, Territory, Population: Lectures at the Collège de France, 1977-1978, trans. by Graham Burchell, ed. by Michel Senellart, François Ewald, Alessandro Fontana, and Arnhold I. Davidson (New York: Picador, 2007), 107-8.
[10] Ibid, 47.
[11] Alan Bewell, “Jane Eyre and Victorian Medical Geography,” ELH 63, no. 3 (1996): 776.
[12] Ibid. See Mervyn Susser and Zena Stein, Eras in Epidemiology: The Evolution of Ideas (Oxford, New York: Oxford University Press, 2009) for more on miasmatic theories of disease.
[13] “During the latter part of the eighteenth century and throughout most of the nineteenth century, ‘medical geography’ was perceived as a knowledge fundamental to the successful expansion of empire. One of the distinctive characteristics of imperial medicine, I would argue, was its mapping of the world, both at the level of localities and larger global territories, in terms of ‘healthy’ and ‘unhealthy’ environments. … Medical geography provided the scientific rationale for making colonial ecologies more like those of Europe, for introducing European methods of land use, social organization, and resource management. The colonization of bodies thus proceeded from, and was largely supported by, the medical colonization of physical space,” Bewell, “Jane Eyre and Victorian Medical Geography,” 780. See also Nicolas B. King, “Securities, Disease, Commerce: Ideologies of Postcolonial Global Health,” Social Studies of Science 32, no 5/6 (Oct-Dec 2002): 763-789.
[14] Tom Koch, Cartographies of Disease: Maps, Mapping, and Medicine (New York: ESRI Press, 2005): 98.
[15] Thrift, Non-Representational Theory: Space, Politics, Affect (New York: Routledge, 2008): 91.
[16] Ibid, 97.
[17] See Mniszewski et al, “EpiSimS Simulation” for more details about the parameters of this particular simulation.
[18] Ibid, 557.
[19] Lakoff, “From Population to Vital System: National Security and the Changing Object of Public Health,” in Biosecurity Interventions: Global Health and Security in Question, edited by Andrew Lakoff and Stephen J. Collier (New York: Columbia UP, 2008): 36.
[20] Ibid.
[21] Lakoff, “Preparing for the Next Emergency,” Public Culture 19, no. 2 (2007): 253.
[22] Ibid.
Lindsay Thomas is a Ph.D. student in the Department of English at the University of California, Santa Barbara. Her research interests include contemporary literature, media studies, and science and technology studies, and her dissertation is on the relationship between security and speculation in speculative fiction and in governmental media and information technologies.
 Media Fields Journal
Media Fields Journal
Reader Comments